Address:
20 Park Plaza, Suite 804
Boston, MA 02116
978-888-7999
Address:
20 Park Plaza, Suite 804
Boston, MA 02116
978-888-7999

Image by Gerd Altmann from Pixabay
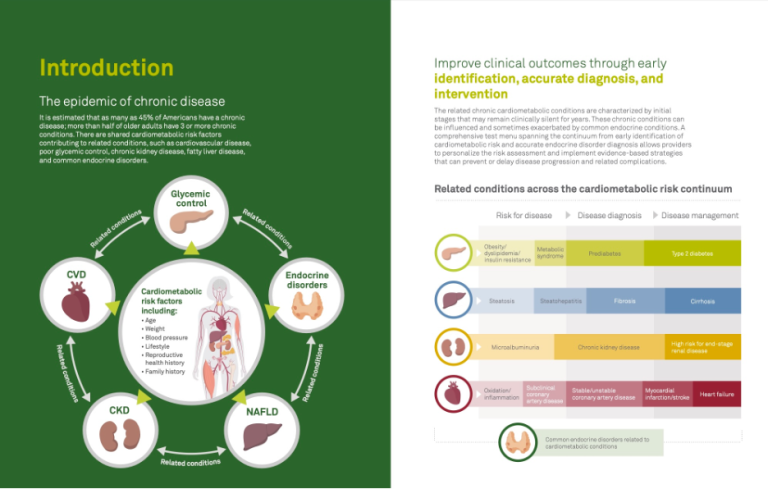
The COVID-19 related collapse of the hospitals in Queens, New York, is burnt into the minds of Americans. Who would be the next person chained to a ventilator? Shockingly, physicians, nurses, EMTs, police, and fire, armed with courage and training, but short of equipment, died along with their patients.
Vaccines are the best long-term solution to COVID-19. A vaccine turns a person into an antibody factory. Once vaccinated, upon exposure to COVID-19 particles, we generate antibodies and killer T-cell that attack the virus. As the virus replicates, each new virion stimulates a more significant response, providing our immune systems are working. Eventually, we neutralize the virus, shortening the duration of the illness while reducing the risk of death or disability. With an effective vaccine, our immune system will respond like this repeatedly over many years. The Warp Speed vaccines all appear safe; the durability of protection for each will only be known in the fullness of time.
Our immune systems make millions of different antibodies (and trillions of varying killer t-cells.) The antibodies produced in the lab only attack COVID-19. Unlike a vaccine, they don’t detect early infection. They don’t create long-term immunity. They cost a hundred times more than a vaccine. One dose contains thousands of times more antibody than we can generate to COVID-19. But given at the appropriate moment, they can overwhelm the virus, preventing progression to hospitalization, intensive care, and death. They are not a cure-all. But with less random outcomes., coronavirus, while undoubtedly serious, will no longer be the stuff of nightmares.
Monoclonal antibodies have been used since 1986 to prevent transplant rejection, cure cancer, and treat connective tissue diseases. They were first used as an anti-viral against the Ebola virus in 2018. Untreated, 75% of Ebola patients die. A cocktail of three monoclonal antibodies, given in the early phase of the illness, reduced the death rate from 75% to 6% (NEJM). Any cure of an Ebola infection is a significant leap in medicine. Side effects were not reported, indicating they were likely mild, which is the case with other monoclonal antibodies. In the world viral warfare, nothing had ever slowed, let alone defeated Ebola.
When asked if monoclonal antibodies like those used for Ebola, could have a significant role in COVID-19, Anthony Fauci, MD, said the antibody treatments were “very encouraging.” However, his laboratory at NIH joined with Eli Lilly to start research on an anti-COVID antibodies back at the beginning g of the pandemic.
Among survivors of COVID-19, many generated significant anti-COVID-19 antibodies. As their health improved (convalesced) they maintained high levels, but soon after the infection was gone, the antibody levels drop. However, convalescent serum differs from monoclonal antibody medications in many ways. Serum must be obtained from a blood donation, it must be screened for infections such as hepatitis and HIV. The non-COVID substances, which make up most of the plasma, can cause allergic and adverse reactions. The FDA approved emergency use of convalescent plasma transfusions from recovered COVID-19 under political pressure and before the Mayo clinic finished its study. Dr. Fauci finds its use problematic. Plasma requires an intravenous infusion, which requires a medical infrastructure not found in many developing countries. Most monoclonal antibody treatments can be administered by a simple injection.

The NIH/Eli Lilly team has recovered a human anti-COVID-19 antibody. Should it work as well as the antibody treatment for Ebola, it would change the trajectory of the sickest of the COVID-19 patients. The plan was to produce monoclonal antibodies thousands of times more concentrated than convalescent serum. Fauci’s conclusion on the proposed monoclonal antibody:
Using an antibody generated by the immune system of a recovered COVID-19 patient gives us a jump start on finding a safe and effective therapeutic. Share on X
Justice Department Leads Where the CDC and FDA Have Failed
Dr. Fauci restricts his observations, with the exception of his critique of his Opening Day pitch at National Stadium, to medical issues, so I can’t say who initiated the request to the Justice Department. However, the history of the supply chain and capacity dilemmas that plagued the CDC’s development of a COVID-19 test was widely known. The consequences of having no testing program include most of the 180,000 COVID-19 related deaths.
The Justice Department ruling should help avoid a similar outcome with the antibody program. They granted six of the largest monoclonal antibody pharmaceutical companies an anti-trust exemption to jointly scale up manufacturing, supply chains, and share scientific information. The exemption can be expanded when more companies apply. In practice, this medication would reduce hospitalizations and deaths. In Ebola, the reduction in deaths was over 85%. Exactly how great the improvement is will come from clinical trials that are already underway. A monoclonal antibody will not end the pandemic, but it should relieve some of our darkest fears.
Press Release: Thursday, July 23, 2020
Department of Justice Issues Business Review Letter to Monoclonal Antibody Manufacturers To Expedite And Increase The Production Of Covid-19 Mab Treatments
(Interview Dr. Fauci NIH press release 8/4/20).